
Business & Motivation
The anti-aging market has long been considered a booming business, and the last few years have seen a notable shift in how we view aging. The hot topic is the distribution of melanin, or pigmentation, in skin as a marker of age.
Of course, fine lines and wrinkles are those old standbys of anti-aging vocabulary, and continue to be of concern to clients worldwide. However, current consumer research indicates that uneven skin coloring – specifically, the blotches and dark spots on the face, décolleté and hands which are a classic indicator of UV exposure and hormonal shifts – now matches or even surpasses concerns about skin smoothness and texture.
Do Ask, Do Tell
As a skin care professional, use your skills to address pigmentation in the context it deserves: as a factual part of the client’s scientific and chemical composition. Knowing ancestry detail will be ideal information when developing their treatment plan.
The color of our skin as an innate aspect of our physiology is hereditary. With modern society being an increasingly rich mix of ethnicities, looking alone does not tell us enough. For a skin-therapist, treating changes in pigmentation is about becoming a bit of a DNA sleuth. We need to ask key questions to help identify what we are observing. During the consultation, take the time to identify clients’ ethnic heritage as specifically as possible:
Appearances can often be deceiving; especially as the years pass, sun exposure and other environmental factors may alter the superficial appearance of the skin. When working with pigmentation, there are always underlying components that may counter-indicate specific treatment.
For example, someone with visibly-light skin may possess ancestry that counter-indicates chemical peels or other aggressive procedures. To get a baseline reading, incorporate a combination of the Fitzpatrick Skin Type Classification Scale for inflammation response and the Lancer Ethnicity Scale for ethnic heritage into skin are consultations.
Common Hyperpigmentation Issues
Analyzing pigmentation is a nuanced aspect of the skin care profession. Begin by familiarizing yourself with these common pigmentation issues, and remember that the client may have several simultaneous conditions.
Drug-Induced Hyperpigmenation (DIH): Although not considered a main factor, changes in pigmentation are usually due to illnesses, certain prescription medications or reactions of the drug. DIH, when observed, takes on a more diffused look. Specific patterns or hues have been observed. For example:
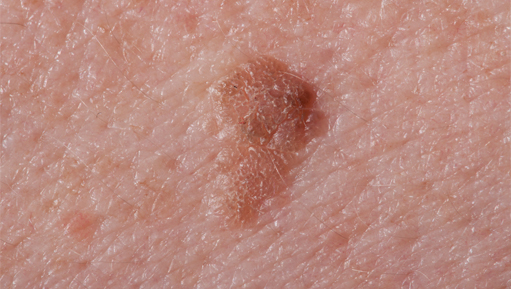
Lentigines: Commonly known as liver spots or age spots, lentigines are benign pigmented spots with a clearly defined edge. While not directly caused by the aging process, they become more prevalent with age. Related more to UV exposure, they are found on 90% of light-skinned individuals over the age of 60. However, they will stay stable in color regardless of sunlight exposure, unlike freckles.
Melasma: Caused by hormonal fluctuations, melasma is common, for example, during pregnancy, with some thyroid dysfunctions, and through use of birth control pills and hormone replacement therapy. One of the most challenging pigmentary conditions to treat, melasma affects more than 5 million Americans. It normally appears on sun-exposed areas of the face and as flat distinct areas of discoloration.
Phytophotodermatitis: A phototoxic reaction that results from sensitivity to ultraviolet light, phytodermatitis is caused by contact with the photosensitizing compounds, specifically furocoumarins found in some plants and vegetables, such as limes, parsley and celery.
Post-Inflammatory Hyperpigmentation (PIH): PIH occurs following an injury, such as burns, friction and even professional skin treatments, including extractions and chemical peels, or from other causes of inflammation such as acne. Traditionally, PIH will resolve and fade over time as the skin regenerates itself but this could take months. PIH is normally the easiest type of hyperpigmentation to treat and generally responds well to treatment.
Choosing Ingredients and Products
Knowing as much as possible about your client means that you will be best-equipped to create a treatment that is safe, as well as successful. It is an irony that deeply pigmented skin often seems to age more gracefully than fair skin – but darker skin is prone to forming pigmentation reactions, including PIH or even raised scarring, such as keloids. A common example of PIH is the formation of darkened razor bumps, or pseudofolliculitis, along the beard-line in men with deeply-pigmented skin.
When designing a brightening treatment, the level of exfoliation in particular must be carefully aligned with the tolerance and anticipated reactiveness of the client’s skin. Recommended for all skin, for the most effective desquamation with the lowest incidence of trauma, are Papaya enzyme (Papain), Pumpkin enzyme, Lactic Acid and Sugar Cane Extract. Salicylic Acid and Trichloroacetic Acid (TCA) can also be used to increase cell turnover, but are more aggressive then the former. Proper education and training should be exercised before performing more advanced treatments.
With the long-term health of the client’s skin in mind, select leave-on products that feature and sometimes combine these ingredients:
The latest agents to fight formation of hyperpigmentation are ground-breaking peptides:
Many topical therapies contain a combination of various ingredients including the above and sometimes corticosteroids to combat skin irritation.
Ingredient knowledge combined with the proper skin assessment will help identify the changes in hyperpigmentation, why it responds to stimuli in the manner that it does, and what professional skin care protocols are appropriate.
Managing Expectations
When addressing hyperpigmentation concerns, it is essential to manage client expectations wisely. In an age of instant gratification and “overnight results,†clients may want a lifetime of sun damage or other pigmentation-related conditions undone as if by magic. Always proceed with caution, and take a conservative and patient approach. Speak candidly with your client, and explain that smaller steps will produce effective results with less risk of further damage.
References:



Get special offers on the latest developments from Front.